ARTIFICIAL INTELLIGENCE SOLUTIONS AND ITS IMPACT IN HEALTHCARE SERVICES – Part II
Author’s note: This article is part of a series published in SeAMK eJournal about cutting-edge technologies (Artificial Intelligence, Big Data, Robotics, and Internet of Things) that will revolutionize the healthcare in the near future.
(Continued from ARTIFICIAL INTELLIGENCE SOLUTIONS AND ITS IMPACT IN HEALTHCARE SERVICES – Part I)
In an ideal application of Artificial Intelligence (AI) system in healthcare the origin and finish must be in the clinical side. Therefore, the action framework should be established in a closed loop where the workflow starts with a clinical need or activity and ends with the use of the system’s outcomes by a healthcare professional (see Figure 1). Therefore, an optimal adoption of AI in the healthcare considers a integrative decision support approach, where the system can actively request clinically relevant information (image, genetic or other structured data) or gather the data from EHR (unstructured data), process it through AI algorithms (Machine Learning or Natural Language Processing) to show the results to clinicians, and if needed write them into EHRs automatically.
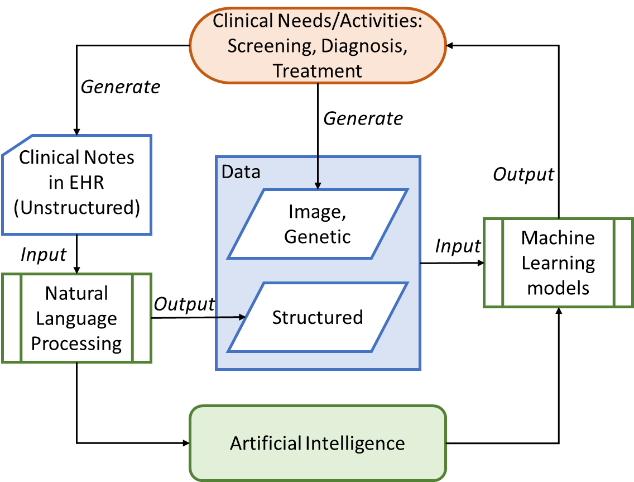
Figure 1: The framework for generating, processing and analysis clinical data using a healthcare AI algorithm [1]
AI solutions that employ algorithms like classical Machine Learning (ML), Deep Learning (DL), natural language processing (NLP) provide their outcomes by processing different data structure. Thus, structured data allows to infer a distinct target attribute (e.g. outcome of a given disease) by supervised learning models applied to other patient’s input features. Conversely, unsupervised learning is employed over unstructured data to extract underlying features from the original source like laboratory reports, operative notes or discharge summaries. However, there are cases, mostly used in healthcare, named semi-supervised learning where unsupervised learning is applied to identify features needed in next supervised learning stages to obtain a compulsory outcomes.
Advantages that AI could bring to healthcare are numerous: enhanced disease detection, personalized medicine, optimization of existing resources, bringing clinical expertise to remote regions, managing time and saving costs. However, real-world clinical implementation of AI has not yet become a reality since there are points to be considered like confidentiality, access authorization and tracking, integrity and availability of patient data; appropriate infrastructure and interoperability of health information systems; and data standards or regulatory frameworks. Moreover, lack of interpretability as well as self-learning bias in the results are other factor that affect the integration in clinical workflow since AI technologies need to be transparent and robust to justify a specific diagnosis, treatment recommendation, or outcome prediction. Thus, not only the healthcare workforce should be educated about AI and understand both its benefits and limitations, but also collaborate interdisciplinary with programmers to ensure the algorithms correspond with the goals of clinicians providing patient care.
Regarding economy aspects, an optimal performance of AI system will require maintenance of increasing amounts of patient data as well as updating complex software algorithms that demands increasingly powerful hardware resources. Thus, funding will be critical to ensure successful implementation although now it is not clear how use of AI technologies will be reimbursed. However, the potential savings thanks to AI are estimated to have a big impact on healthcare industry, for instance $ 150 billion in annual saving for the U.S economy by 2026 [2].
At the current AI research and development phase the replacement of human doctors will not take place, and not unless “AI singularity” occurs [3], because in part those superior performances in the theoretical setting has not translated well into real-world clinical practice. Moreover, there are areas like emotional support and rapport where the nature of the clinicians-patient interaction is hardly achievable and fundamentally different through AI-based technologies. Although AI may perform certain routine tasks like diagnostic tests that involve pattern recognition (e.g. pathology and radiology) with greater consistency, speed, and reproducibility than humans, the hope is that AI may augment the ability of humans to provide a more precise and personalized healthcare. Human doctors can also use their intuition that is trained over years of experiences to oversee the working of AI algorithms. Furthermore, by automating tasks which are not theoretically complex but can be incredibly labor, cost and time-intensive, doctors may be freed to tackle more complex tasks, representing an improved use of human capital. The implementation of AI-based technologies in healthcare will provide no shortage of work for the future. Nevertheless, the discharge decision or diagnosis/treatment confirmation should rely always on the doctor’s evaluation and assessment of patient’s condition since the priority in the use of AI is the patient safety. Around the patient safety requirement, the “accountability” issue should be legally tackled, because AI as humans is not infallible: if a patient suffers an adverse event due to an AI-based technology, who is responsible?
Pedro A. Moreno Sánchez
RDI Expert/ Researcher
PhD, PMP®
Seinäjoki University of Applied Sciences
School of Health Care and Social Work
References
[1] M. Alloghani, D. Al-Jumeily, A. J. Aljaaf, M. Khalaf, J. Mustafina, and S. Y. Tan, “The Application of Artificial Intelligence Technology in Healthcare: A Systematic Review,” in Applied Computing to Support Industry: Innovation and Technology, Cham, 2020, pp. 248–261, doi: 10.1007/978-3-030-38752-5_20.
[2] S. Latif, J. Qadir, S. Farooq, and M. A. Imran, “How 5G Wireless (and Concomitant Technologies) Will Revolutionize Healthcare?,” Future Internet, vol. 9, no. 4, p. 93, Dec. 2017, doi: 10.3390/fi9040093.
[3] R. Kurzweil, The singularity is near: When humans transcend biology. Penguin, 2005.
[4] J. He, S. L. Baxter, J. Xu, J. Xu, X. Zhou, and K. Zhang, “The practical implementation of artificial intelligence technologies in medicine,” Nat. Med., vol. 25, no. 1, pp. 30–36, Jan. 2019, doi: 10.1038/s41591-018-0307-0.
[5] K.-H. Yu, A. L. Beam, and I. S. Kohane, “Artificial intelligence in healthcare,” Nat. Biomed. Eng., vol. 2, no. 10, pp. 719–731, Oct. 2018, doi: 10.1038/s41551-018-0305-z.
[6] E. Loh, “Medicine and the rise of the robots: a qualitative review of recent advances of artificial intelligence in health,” BMJ Lead., vol. 2, no. 2, pp. 59–63, Jun. 2018, doi: 10.1136/leader-2018-000071.
[7] R. Miotto, F. Wang, S. Wang, X. Jiang, and J. T. Dudley, “Deep learning for healthcare: review, opportunities and challenges,” Brief. Bioinform., vol. 19, no. 6, pp. 1236–1246, Nov. 2018, doi: 10.1093/bib/bbx044.
[8] F. Jiang et al., “Artificial intelligence in healthcare: past, present and future,” Stroke Vasc. Neurol., vol. 2, no. 4, pp. 230–243, Dec. 2017, doi: 10.1136/svn-2017-000101.